Ever since I became a fitness instructor back in 1997, I was assured by every trainer and every therapist I met that pain can simply be stretched away.
In practice, results are far more mixed. Whether people are doing the wrong stretch, for the wrong time, or lying , if you are honest, stretching often isn’t a long term solution for pain.
I wrote about this in my “backaholic” blog where I quoted some of the observations made by Stuart McGill And Boo Schexnayder
“Soft tissue injuries result from excessive tension, so excessive tension in the rehabilitation situation is counterproductive…stretching of …chronically tight tissue is counterproductive. It may give an initial sensation of relief because the muscle spindles have been deadened, but this practice…weakens the tissue further because of the weakened proprioceptive response.” Boo Schexnayder
“stop trying to Stretch and mobilise! Let tissues settle and regain their proprioceptive abilities so they tell the truth” Stuart McGill
Its important to recognise that stretching has an analgesic effect , but it seems to be attributed to switching receptors off in the muscle. ( I suppose its like I’ve cured your headache by switching off the fire alarm, but I haven’ checked that there isn’t a fire!!).
Do bear in mind that pain has many causes. I have clients with bad backs, caused by rubbish abusive employers, I have clients who use their backs appallingly, and are so tight their posture is disgusting, who have never had a minutes worth of pain.\
Nevertheless stretching has enough of an albeit , muddled, pedigree to justify its inclusion in pain treating especially if better protocols can be designed.
In the therapy world, the chances are we know everything, it’s probably a matter of nailing the sequencing to get optimal results.
We know for example not to train static stretching before sprint practice. “in strict terms of performance, it seems harmful to include static stretching in the warm-up protocol of collegiate male sprinters in distances up to 100 m”. (ref)
So what do we have to do to make stretching work as a pain relieving protocol? Because just to say ” stretching is magic” doesnt cut it :
If you read “Effectiveness of calf muscle stretching for the short-term treatment of plantar heel pain: a randomised trial”. (Ref) they found that “When used for the short-term treatment of plantar heel pain, a two-week stretching program provides no statistically significant benefit in ‘first-step’ pain, foot pain, foot function or general foot health compared to not stretching.”
Well check out Effectiveness of Myofascial Trigger Point Manual Therapy Combined With a Self-Stretching Protocol for the Management of Plantar Heel Pain”
This 2011 study combined trigger point therapy with stretching and concluded “that the addition of TrP manual therapies to a self-stretching protocol is superior to the sole application of self-stretching in the treatment of individuals with plantar heel pain at short term“.
So its really worth thinking about combining trigger point therapy with stretching.
If you want to get an inexpensive handle on trigger points, buy this book

If you are near the east end of london, you can book a PT session with me and ill show you how (andrew@andrewstemler.com)
So, for now, my conclusion is that, when apply stretching for pain relief, it’s sensible to consider combining Trigger points with stretching. I’ll talk about the re education of tissues, rest period, elsewhere.
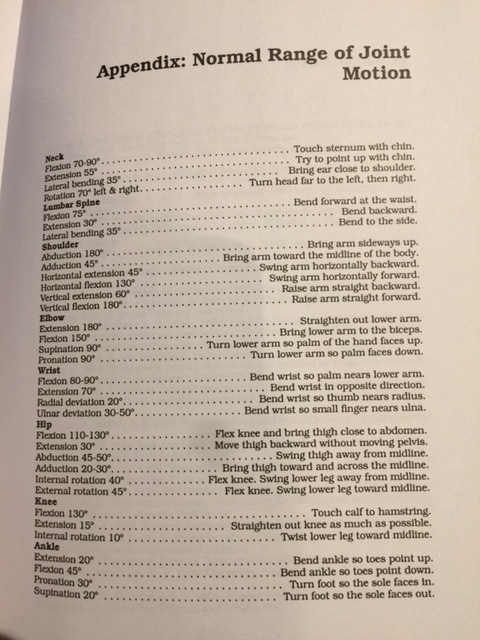
It’s still important to say that every year dancers, gymnasts athletes and physical enthusiasts get flexible by using a mix of the work of Zaichik, Kurz and others. That you can improve your range of motion isn’t really up for debate.